Michael Chizner, MD wrote a great article in July 2008 on the lost art of listening to the heart called:
Cardiac Auscultation: Rediscovering the Lost Art - It is great. Listening for murmurs is a difficult skill to master. I have worked with several seasoned PAs and MDs that still claim that they don't have a good handle on murmurs. Personally, I am terrible at it. I can tell you it is abnormal and I can tell you what the text book systolic or diastolic murmurs should sound like.... but hearing a heart beating at 80 bpm and picking out and correctly naming a murmur.... I'm definitely not there yet.
If you have access to your school's library- you should have access to free journal articles. Just do a quick search for the title and author. Below is a snippet from the article.
TABLE 1. Proper cardiac auscultatory technique
● Room should be quiet
● Time heart sounds and murmurs by “inching” technique (or by palpation of carotid artery
or apical impulse)
● The bell of the stethoscope is best for low-frequency sounds and murmurs (eg, S4 and S3
gallops, diastolic rumbles)
● The diaphragm of the stethoscope is best for high-frequency sounds and murmurs (eg,
aortic regurgitation)
● Listen with bell lightly applied at cardiac apex, with patient turned to left lateral decubitus
position, for S4and S3 gallops and/or diastolic rumble of mitral stenosis
● Listen with diaphragm firmly applied over the left sternal border with patient sitting
forward, during held expiration for diastolic blowing murmur of aortic regurgitation and/or
pericardial friction rub
● Listen individually to S1 and S2
— Are both S1 and S2 present?
— Is either sound loud, normal, or faint? Does splitting of S2 widen, remain “fixed,” or
reverse with inspiration?
● Listen for extra sounds in systole (eg, mitral clicks, aortic or pulmonic ejection sounds)
or diastole (eg, S4 and S3 gallops, pericardial knock sound, mitral opening snap, “tumor
plop”)
● Listen for murmurs
— Systolic (early, mid, late, holosystolic)
— Diastolic
— Continuous
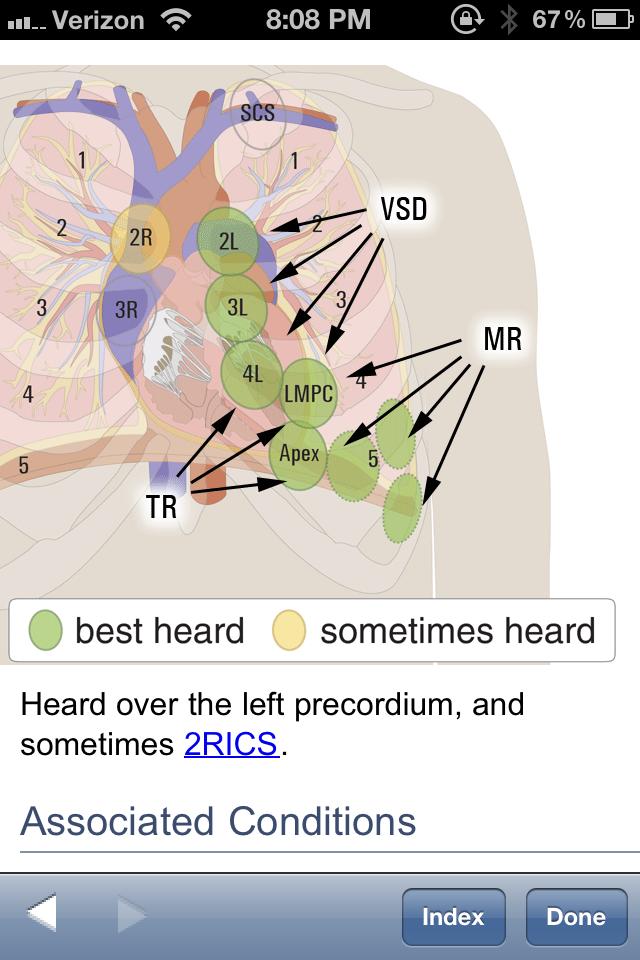
— Where is the murmur heard and radiate?
— Does the murmur change with body position, respiration, certain maneuvers (eg,
Valsalva)
Listen for pericardial friction rubs or prosthetic valve sounds
(Reproduced with permission from Chizner MA. Clinical Cardiology Made Ridiculously Simple, 2nd edition. Miami, FL: MedMaster, Inc., 2007.)
Picture: http://www.medcomrn.com/cgi-bin/mc/sectionpreview?8a9dQUaN;VIDM259B-T;620